HEART Pathway for Early Discharge in Acute Chest Pain
Identifies emergency department patients with acute chest pain for early discharge.
- Use in patients ≥21 years old presenting with symptoms suggestive of acute coronary syndrome (ACS).
- Do not use in patients with new ST-segment elevation ≥1 mm, hypotension, life expectancy <1 year, or a noncardiac medical/surgical/psychiatric condition determined by the clinician to require hospital admission.
Advice
- The HEART Pathway is an accelerated diagnostic pathway (ADP) and is not intended to replace clinical judgment.
- Any patient with a concerning presentation or clinical progression should undergo further evaluation and treatment at the clinician’s discretion, regardless of the HEART Pathway’s predicted risk.
- Shared decision-making is a critical component of management after ACS risk stratification, particularly for patients at moderate risk who are recommended for observation and comprehensive cardiac evaluation.
- Hospitalization carries inherent risks, as does false-positive or non-diagnostic testing, which may lead to unnecessary invasive procedures such as cardiac catheterization.
- Patients should be counseled on the risk of both missed ACS and hospitalization for additional workup.
- Risk-specific decision aids (e.g., Chest Pain Choice Decision Aid from Mayo Clinic) may be helpful.
- Any patient discharged after evaluation for chest pain should be informed that, despite a negative workup, a small residual risk of ACS remains.
- For patients with a <1% risk of ACS within 30 days, it is important to emphasize that automatic outpatient cardiac risk stratification carries a higher likelihood of false-positive than true-positive results, which may lead to unnecessary invasive procedures with associated risks.
- Instead, patients should be set up with close primary care follow-up and explicit return precautions.
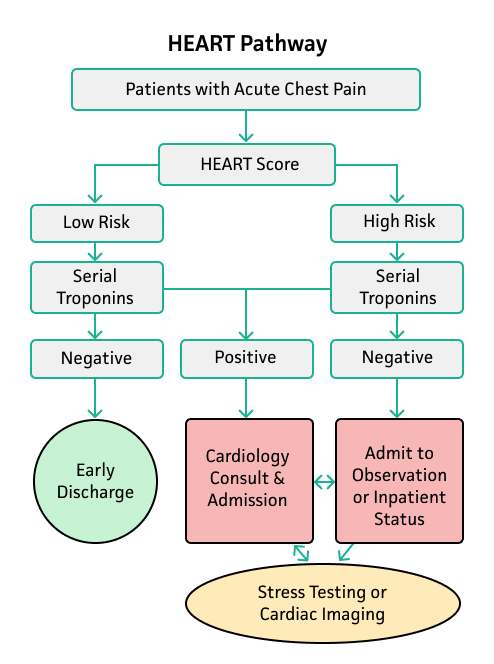
Management
- Low risk patients: Those with a follow-up troponin obtained 3 hours after ED presentation can be considered for safe discharge home with appropriate outpatient follow-up.
- High risk patients: Admit or observe with serial ECGs, cardiac biomarkers, and/or cardiology consultation.
From Mahler 2015.
Critical Actions
- Clinician judgment should supersede results, even when patients are classified as low risk.
- If other features raise concern for ACS, further evaluation should be individualized to the patient.
- All patients presenting to the ED with chest pain concerning for ACS should receive aspirin contraindicated (e.g., known allergy, active bleeding, or receipt of a therapeutic dose prior to arrival).